The administration of testosterone in men over 40 has been proven to be a major anti-depressant, which contributes to anti-aging.
Testosterone maintains the muscular system, provides a more elastic skin, enhances libido and promotes self confidence.
The thoughts become more decisive, while women are attracted to men with high testosterone, through their skin odor.
Hormone replacement with testosterone (TRT) and DHEA has positive effects on reducing the abdominal fat and insulin resistance.
The increase of the abdominal fat promotes the creation of the metabolic syndrome, as well as insulin resistance promotes the creation of lipogenesis (a predisposing factor of diabetes mellitus type II, non insulin dependent).
Considering the fact that testosterone’s biosynthesis initiates from another steroid molecule, cholesterol, it is reasonable why diets low in saturated fats will have a negative impact on its endogenous production.
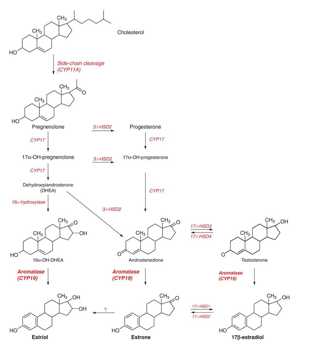 Biosynthesis of testosterone molecule
Biosynthesis of testosterone molecule
Modern medication as statins, lower total cholesterol and low density lipoprotein LDL.
The final result would be to lower total testosterone’s serum levels as well.
Biosynthesis of cholesterol is a process that takes place in the liver parenchyma.
The Leydig cells of the testicles produce approximately between 7-10 mg of the hormone on a daily basis.
This translates into approximately 50-70mg on a weekly basis; roughly ten to twenty times lower, than the abuse of a competitive bodybuilder.
Just by this fact, we understand the degree of atrophy testicles undergo.
It makes sense that after years of AAS abuse, the male ends up hypogonadic for life.
A crushed libido and oligospermia, along with increased body fat, low self confidence, poor muscularity and loss of muscle endurance-strength are present.
Not to neglect the negative consequences of a chronic overdose-abuse on the myocardium, the atheromatic index, the prostatic hypertrophy, polycytemia, androgenic alopecia.
Last but not least, the effects on mental health.
This is the price every competitive or recreational bodybuilder has to pay eventually.
Slow esters of testosterone (enanthate, cypionate) are released gradually, reaching a peak around day four and remaining in the body for a prolonged timing (7-10 days). Aromatization is easier to occur, as a result of this longer half life.
The clinical symptom of gynecomastia is an aesthetic issue, where the nipple is swollen and painful-touchy under palpation.
Enanthate and cypionate esters, release a smaller amount of active testosterone, around 70%.


Greek testosterone enanthate, 250mg/ml Testosterone cypionate, USA, 200mg/ml
In contrast, fast esters (propionate, suspension) have very immediate results, with the disadvantage that they have to be administered more often.
Every other day for the propionate and on a daily basis for the water-soluble-suspension, ester-free form.
They provide a greater amount of testosterone (80% and 100% respectively).
Therefore, testosterone suspension is the most powerful type among injectable testosterones.
Fat acting esters have a lesser chance for aromatization, as a result of their short half life into the body.
They are preferably used during a precontest preparation.
However it should be noticed, that the more estrogenic an AAS is, the greater anabolic properties it has.
Afterall, aromatization and water retention is a fundamental biochemical environment that supports muscle growth and strength.
Testosterone is converted into estrogen, by the enzyme aromatase in mammary gland, adipose-fat tissue, liver and brain.
Obese individuals have elevated levels of (E2) beta estradiol, as a result of greater body fat percentage.
Fast acting testosterone propionate (Danish), Immediate release of water based
100mg/ml testosterone suspension (Indian), 25mg/ml
Testosterone applied in the form of gel, increases the serum levels of dihydrotestosterone (DHT), since the skin has increased concentration of 5a reductase enzyme.
The transdermal absorption of testosterone has only 10% absorbency, but the advantage of sustained release and stable blood levels, compared to the intramuscular (IM) use.
Parenteral (intramuscular) type of administration acts acute into the circulation.
The subcutaneous (SC) use has a delayed absorption and this is why insulin is usually administrated under the skin.
Somatropin (HGH) is administrated subcutaneously because of its lipolytic (fat burning) ability, that also provides a delayed absorption time.
Greek testosterone in gel form 1% Greek testosterone in gel form 2% Greek decanoate testosterone
in oily capsules
During a steroid cycle, the ration between androgens and anabolics, should be (2:1)
This will ensure, there is no crush on libido and sexual drive.
Testosterone has the ability to suppress the production of catabolic cortisol (the main corticosteroid).
This is the reason after the end of a cycle, both cortisol and estrogens rebound and rise dramatically.
As a result of it, the physique gets smooth and muscle wasting occurs (catabolism).
The use of anti-estrogenic compounds (tamoxifen, anastrozole, letrozol, exemestane) has a negative impact on testosterone’s benefits, regarding muscle growth. Tamoxifen citrate is known to suppress IGF1 in liver.
On the other hand the significance of the estrogenic environment to muscle growth is fundamental.
Estrogens enhance muscle glycogen synthesis, through water retention.
Therefore, muscle strength and stamina is enhanced.
Estrogens are known to improve steroid receptors affinity to the steroid molecules.
Estrogens improve joints lubrication, by retaining water into the synovial cavity.
This is something critical under off season heavy duty training.
A proof that women produce testosterone, but a lesser amount than men, is the fact that older women have increased facial hair, known as hirsutism.
This practically occurs after the menopause when estrogens are no longer produced. Androgens produced by the adrenal glands and ovaries, continue their action, and therefore manifest their androgenic secondary characteristics.
Androgens can act therapeutically, though, for a woman in the case of breast cancer.
The estrogens are in exacerbation, so androgens (fluoxymesterone) act as an alternative treatment.
Nowadays, under the new generation of anti-estrogens (anastrozol, letrozol, exemestan), the use of 17 alkalized hepatotoxic AAS is no longer necessary.