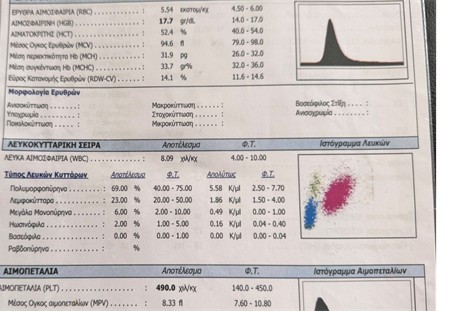
Patient with Polycythemia Vera (gene mutation JACK II).
Observe the elevated thrombocytes (490000 μL) with high hemoglobin (17.7 g/dL) -Fig. 1
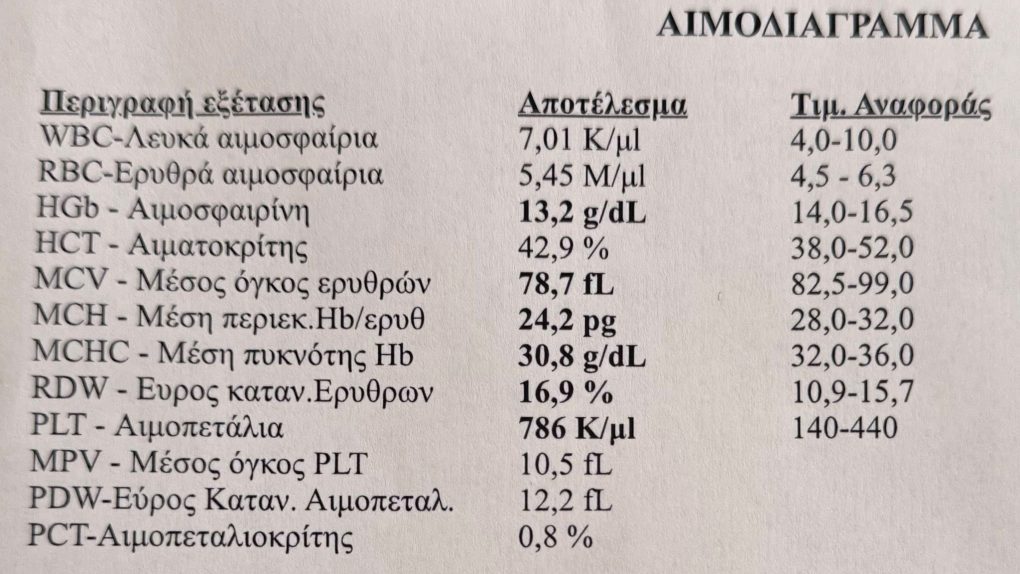
Patient undergo repeated phlebotomies, that eventually dropped his hematocrit and hemoglobin to very low levels (tanked ferritin and iron, causing horrible fatigue).
Notice the remarkable elevation of platelets from 490000 μL to 790000 μL (Fig1, Fig 2).
This phenomenon verifies, what I’ve been saying about the compensation of bone marrow in regards to hemoglobin and platelets.
When hematocrit is high (such as with testosterone, Obstructive Sleep Apnea – OSA, high altitude, or even smoking), the system compensates and regulates a balance between Hematocrit/Hemoglobin and platelets.
Vice o, when we undergo blood donations, the opposite happens and as Hematocrit/Hemoglobin drop, thrombocytes elevate.
The take home message is that in secondary (and not primary erythrocytosis as Polycythemia Vera), there is no risk of clotting.
And even if are Hematocrit/Hemoglobin >18/54, platelets will be regulates by a compensatory mechanism.
In terms of prevention, salicylic acid & DHA/EPA will ensure de activation of platelets, throughout an invitation of prostaglandins.