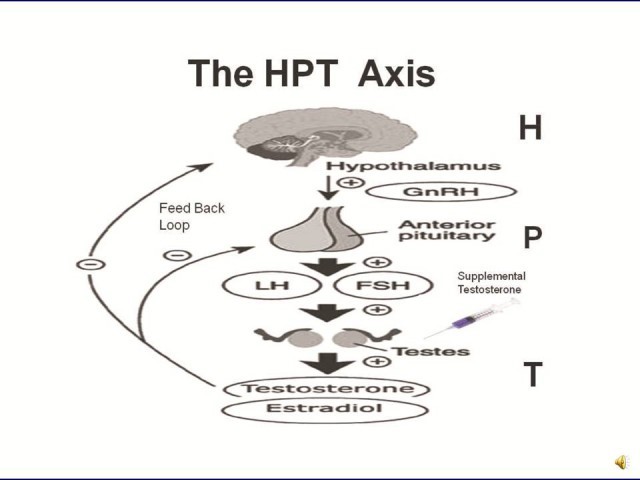
 In men, there is a homeostatic mechanism that interacts between hypothalamus-pituitary-testicles the Hypothalamic Pituitary Testicular Axis (HPTA), which is regulated interactively.
In men, there is a homeostatic mechanism that interacts between hypothalamus-pituitary-testicles the Hypothalamic Pituitary Testicular Axis (HPTA), which is regulated interactively.
Hypothalamus interacts with hypophysis, the pituitary gland located at the sella turcica of the sphenoid bone and gonads (testicles), adjusting their operation.
Androgenic anabolic steroids (AAS) are synthetic derivatives of testosterone, the main androgen. Testosterone itself significantly suppresses the HPTA axis, while several other derivatives induce the suppression into a greater or lesser extent.
AAS are classified into three main categories:
- Derivatives of testosterone (boldenone, fluoxymesterone, methyltestosterone)
- Derivates of dihydrotestosterone-DHT (stanozolol, methenolone, oxandrolone, oxymetholone) and its synthetic forms (mesterolone, drostanolone)
- Derivatives of the 19-nortestosterone (nandrolone, trenbolone)
Factors that contribute to the suppression of the HPTA axis are:
- The origin of the AAS
- Their degree of aromatization, namely their ability to produce estrogen (E2), through the aromatase enzyme in certain tissues (adipose tissue, mammary gland)
- The duration and dosage of AAS abuse
- The androgenicity of the particular AAS
AAS that cause the greatest suppression of the HPTA axis are:
- Testosterone derivatives.
Testosterone itself, suppresses the axis from the very first day of use.
- Highly aromatized AAS.
E2-beta estradiol provides a negative feedback to hypothalamus for GnRH production, that in turn will increase the production of LH (and testosterone) from the Leydig cells of testicles. Therefore, the AAS that aromatize or have a high affinity for the ER, (oxymetholone?, methyltestosterone, nandrolone, testosterone, methandienone), will suppress HPTA axis.
Another reason why estrogens decrease the libido is the fact that, they increase the concentration of the sex hormone binding globulin (SHBG), which binds testosterone and leaves a small percentage to be released free as active form (FT).
- Progestin AAS.
The derivatives of 19-nortestosterone have high progestational activity.
This mainly occurs, under the presence of aromatisation and high beta estradiol concentration.
Prolactin is a hormone released by frontal-anterior pituitary lobe, or adenohypophysis.
It is inversely proportional to the production of testosterone.
Therefore, prolactinemia will lead to suppression of the HPTA axis.
- Potent androgens (fluoxymesterone, trenbolone, methyltrienolone).
These drugs have a strong binding affinity to the androgen receptor (AR) in the brain.
AAS cross the blood-brain barrier and bind tightly to the AR in hypothalamus (master gland in midbrain).
This results in a greater suppression of the HPTA axis.
The androgenic activity-androgenicity of AAS is responsible for the development of the primary and secondary sexual characteristics (growth of testicles, scrotum, penis, prostate, pubic hair, voice deepening-hoarseness and the development of sebaceous glands).
Other biological actions of androgens include:
– Enhancement of erythropoiesis (by promoting erythropoietin synthesis in the kidney and by increasing erythroid colony-forming units in the bone marrow and promoting their differentiation into erythropoietin-responsive cells).
– Anabolic effect, i.e the increase of muscle mass and strength, increasing the size of muscle fibers. The administration of testosterone leads to positive nitrogen retention and increased protein synthesis.
– Lipolysis (beta-oxidation of adipose tissue) by reducing abdominal fat, leading to lower the insulin resistance-increased sensitivity.
According to Dr.Michael Scally, author of book: “A question of muscle”, AAS (that do not aromatise) could become the solution against obesity.
– Impact on the CNS with neurodegenerative effect, induction of apoptosis in hippocampus and enlargement of the amygdala.
Amydgala along with hippocampus belong to the limbic system, which determines the emotional status.
Clinical symptoms of AAS neurotoxicity include aggression, hypomania-mania, depression, bipolar disorder, psychotic behavior (misconceptions, delusions, and hallucinations)
AAS with high androgenic index usually have high activity of 5a-reductase enzyme and the produced DHT will mainly affect the prostate (hypertrophy-BPH) and scalp (alopecia-MPB).
The DHT derivatives do not aromatize, thus don’t lead to any water retention, or edema.
Therefore, no beta estradiol (E2) is elevated, being responsible for the suppression of the HPTA axis (GnRH negative feedback)
DHT is a potent androgen in the body (five times stronger than testosterone) and also suppressive to HPTA axis.
At the same time, it is also anti-estrogenic, when applied topically (locally applied to male nipples having gynecomastia).\
Another fact demonstrating the antiestrogenic effect of DHT is when the use of 5a-reductase inhibitors (finasteride, dutasteride) for the treatment of prostatic hypertrophy or male pattern baldness.
Men, who use this medication, later observe gynecomastia, depression and lack of libido.
DHT is a strong androgen, after all.