 The intake of androgenic anabolic steroids (AAS) burdens the kidneys through the process of glomerular filtration in the renal parenchyma.
The intake of androgenic anabolic steroids (AAS) burdens the kidneys through the process of glomerular filtration in the renal parenchyma.
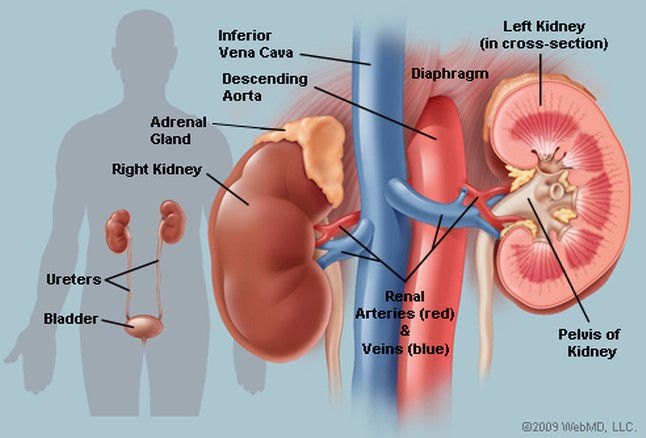
The first stage of AAS metabolism takes place into the liver, but later chemicals pass through the glomerulus and renal tubules (proximal & distal) to be excreted.
The creatinine serum level, which is a reliable indicator of renal function, increases (> 1.5mg/ dl), as well as urea (>50 mg/ dl) and uric acid (>7.5 mg/ dl).
It should be noted that, all these biochemical parameters are affected from several other non-renal factors (state of hydration, vegan diet) and their levels will not be raised above the normal range, until 60% of total kidney function is lost.
So, the most reliable indicator of renal function is the measurement of creatinine clearance (GFR) at 24hrs.
Trenbolone is highly nephrotoxic, gives a characteristic brown color urine and should not be combined with other aggravating substances for the kidney, such as non-steroidal anti-inflammatory drugs-NSAID’s (diclophenac, dimesulid), antibiotics (aminoglycosides) and diuretics (furosemide).
The abuse of trenbolone-stanozolol stacking has been associated with severe cholestasis and acute renal failure (ARF).
Findings of renal biopsy reveal a direct toxic effect on glomeruli and renal tubules resulting in focal segmental glomerulosclerosis, tubular necrosis, nephrotic syndrome and eventually ARF.
Clinically, the patient presents with edema in the face and lower extremities (from proteinuria, hypoalbuminemia), hypertension, oliguria or even anuria (urine volume<500ml/24h).
In microscopic urinalysis proteinuria, microhematuria and cylinders are present.
Besides AAS abuse, athletes have additional factors that could exert stress on renal function, such as overtraining, creatine monohydrate supplementation, high protein intake, elevated BMI (>30) and dehydration.
– During intense over training, where rhabdomyolysis appears (increased serum CPK>1000), damaged muscle fibers release myoglobin, a protein responsible for carrying oxygen to skeletal muscles.
This protein is nephrotoxic for renal glomeruli and tubules and may lead to acute tubular necrosis and ARF.
Kidney function impairment from rhabdomyolysis presents with a dark color of the urine, microscopic hematuria (pinkish, red color), proteinuria or the presence of cylinders.
A dark brownish color of the urine is also a feature of liver/ biliary disease, as a result of cholestasis from AAS abuse.
This pigmentation is due to urobilirogen, coming from excess conjugated bilirubin (bilirubinuria).
– The use of creatine monohydrate in the form of a supplement, or through the consumption of red meat (high protein intake of >300 g/day) increase glomerular filtration rates and is associated with focal segmental glomerulosclerosis and acute tubular necrosis.
Creatine monohydrate with loading doses of 20 g/day for 5 days and then maintenance doses of 5 g/day are considered to be safe, always with proper hydration.
During precontest preparation and glycogen depletion phase, the high consumption of animal protein (>3gr/kg), increases serum levels of ammonia (ammonemia), which is a waste product in urea cycle.
Ammonia gives skin and sweat a characteristic heavy odor and is toxic to brain’s function (hepatic encephalopathy).
Moreover, high protein consumption produces acidic (<5) urine pH, while vegetarian diet with increased fruits and vegetables result in an alkaline (> 7.0) urine pH.
That, along with increase of calcium retention (nandrolone abuse), could lead to hypercalcemia and formation of kidney stones.
Nephrolithiasis can cause direct injury to the kidney and plugging of the ureters, especially under dehydration state (urine specific weight >1030).
Protein consumption tends to be diuretic, in the absence of carbohydrates and in such cases ketosomes are detected in a biochemical analysis, leading to exhalation of ketones (rotten apple smell).
– Greater body mass (BMI> 30) leads to higher glomerular hyper-filtration, which in time leads to mechanical strain and scarring.
Furthermore, studies have found that chronic hyperfiltration from a high-protein diet may accelerate progression to glomerulosclerosis.
In rare cases, abuse of AAS has been associated with the development of kidney tumors (Wilm’s tumor or nephroblastoma).
It is well known that, kidneys regulate arterial blood pressure through rennin–angiotensin-aldosterone system.
Abuse of CNS stimulants such as beta-agonists (clenbuterol) or ephedrine leads to vasoconstriction of renal vessels, chronic systemic hypertension, proximal and distal tubular necrosis and acceleration of renal failure.
Diuretics also have a negative impact on renal function, particularly when their abuse is accompanied by water restriction.
The abuse of performance-enhancing drugs (PED’s) adversely affects renal function through direct and indirect mechanisms.
Firstly, AAS are nephrotoxic and associated with the development of focal segmental glomerulosclerosis and tubular necrosis.
On the other hand, rhabdomyolysis, high protein and creatine intake, nephrolithiasis, inadequate hydration and high incidence of polypharmacy are other factors that contribute to a rapid decline in renal function.